
There has been an increasing interest in the electrocardiographic pattern of early repolarization in recent years following the publication of a paper by Haissaguerre and colleagues in 2008, which linked their definition of the pattern to sudden cardiac arrest due to idiopathic ventricular fibrillation. However, earlier and later publications by other groups on the topic
There has been an increasing interest in the electrocardiographic pattern of early repolarization in recent years following the publication of a paper by Haissaguerre and colleagues in 2008, which linked their definition of the pattern to sudden cardiac arrest due to idiopathic ventricular fibrillation. However, earlier and later publications by other groups on the topic of early repolarisation seemed to exhibit disagreement over what constituted the ECG pattern of early repolarisation suggesting a degree of confusion following the 2008 publication
There has been an increasing interest in the electrocardiographic pattern of early repolarization in recent years following the publication of a paper by Haissaguerre and colleagues [1] in 2008, which linked their definition of the pattern to sudden cardiac arrest due to idiopathic ventricular fibrillation. However, earlier and later publications [2-17] by other groups on the topic of early repolarisation seemed to exhibit disagreement over what constituted the ECG pattern of early repolarisation suggesting a degree of confusion following the 2008 publication [1].
In 1947, Myers et al [2] reported that, among other features, an “elevation of the RS-T take off of 0.5 – 2.0mm may be considered as a normal variant” provided that the ST segment was concave upwards and followed by a tall T wave. In 1951, Goldman also reported on RS-T segment elevation in V3-V6 as a normal variant [3].
The original description of what for many years was regarded as the early repolarization pattern can probably be traced back to an early paper by Wasserburger and Alt [4] dealing with normal RS-T elevation in the relatively newly established full 12 lead ECG. The authors pointed out that the ST elevation mostly arose from a distinct notch on the downslope of the R wave but was occasionally associated with a “well-defined slur”. It is interesting to note that the authors commented that “failure to recognise this pattern as a normal variant …..may result in irreversible iatrogenic heart disease with all its attendant economic and social repercussions”.
Grant et al [5], in a study of the characteristics of the “S-T and T vectors” made reference to “normal early repolarization forces”. They also referred to significant deviations of S-T segments in normal subjects and their reference to normal early repolarisation forces could be interpreted simply as electrical activity in the early part of the repolarisation process rather than what might be regarded as premature repolarisation.
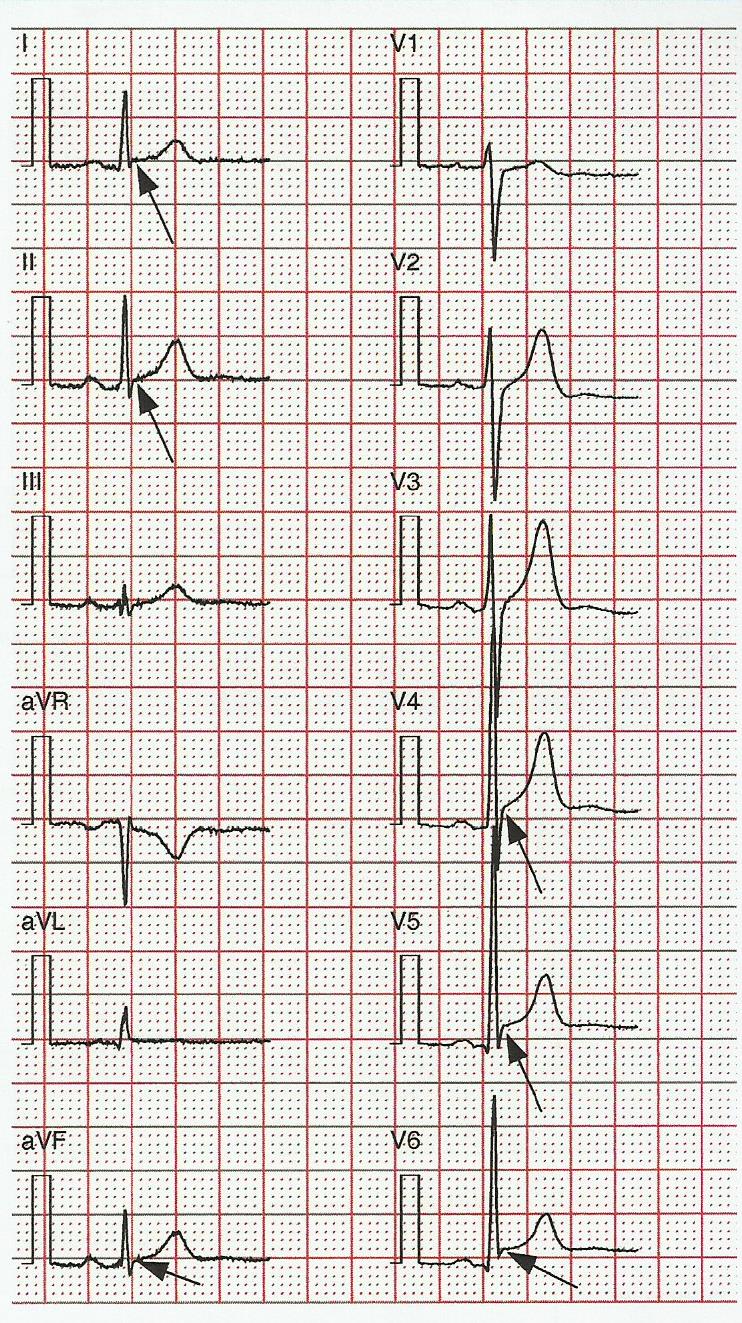
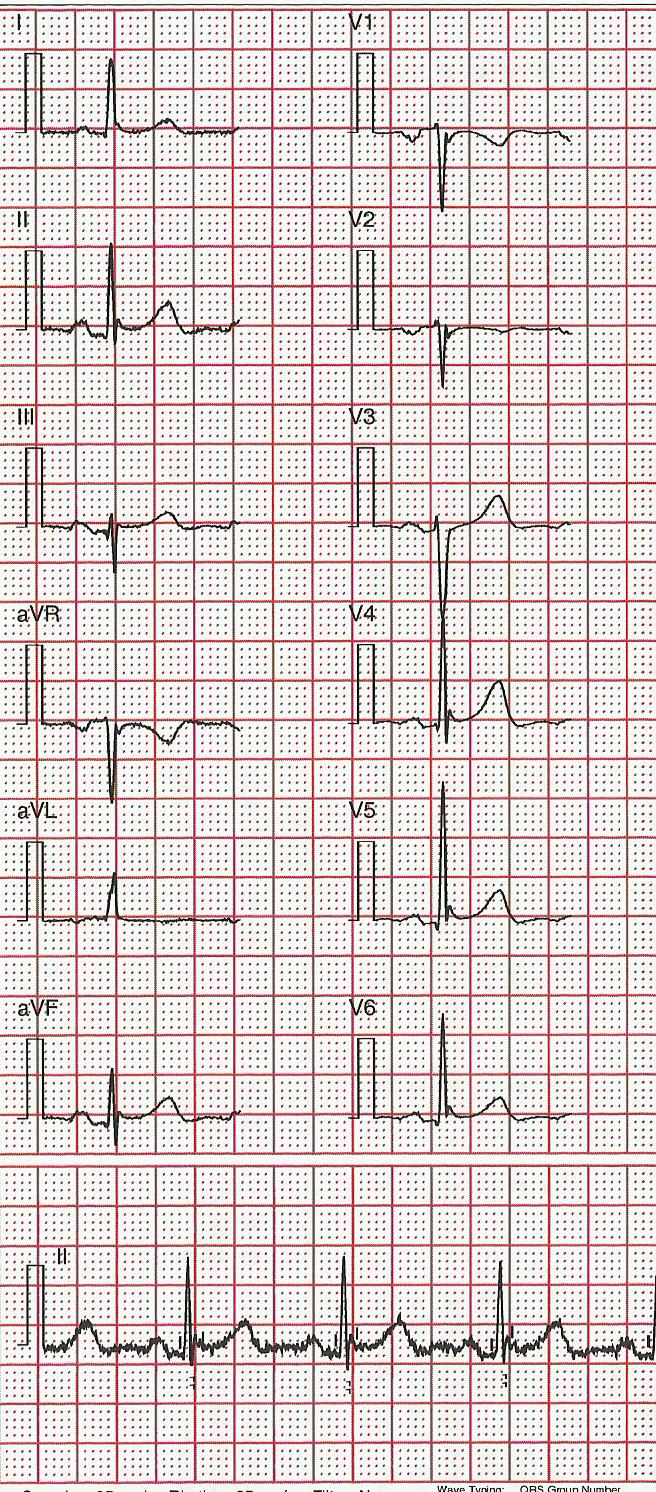
It fell to Kambara et al in 1978 to formulate the criteria of Wasserburger and Alt in a tidy fashion [6] and define the early repolarisation pattern as the grouping of an elevated J point, a distinct notch or slur on the downstroke of an R wave, upward concavity of the ST segment and a symmetrically tall T wave. At that point, reference to notching and slurring on the downstroke of the R wave seemed to gain importance in the definition of early repolarization (ER). However, these authors probably mistakenly introduced the term “early repolarisation syndrome”. In their case, “syndrome” referred to a combination of ECG features and bore no relationship to a clinical syndrome involving life threatening arrhythmias. These authors also did not clearly indicate what they meant by J point but it can be assumed that, in 1978, it meant the onset of the ST segment. Figure 1 shows a “classic” early repolarisation pattern particularly as seen in V4, V5.
Figure 1.
.
Classic early repolarisation pattern in V4 and V5 with an end QRS notch and slur along with some ST elevation.
The ECG pattern is often simplified by describing it as the difference between two action potentials, such as an endocardial and an epicardial action potential. If the epicardial action potential commences “early”, then it is possible to show (Figure 2) on this model that a notched QRS complex may arise [7].
Figure 2
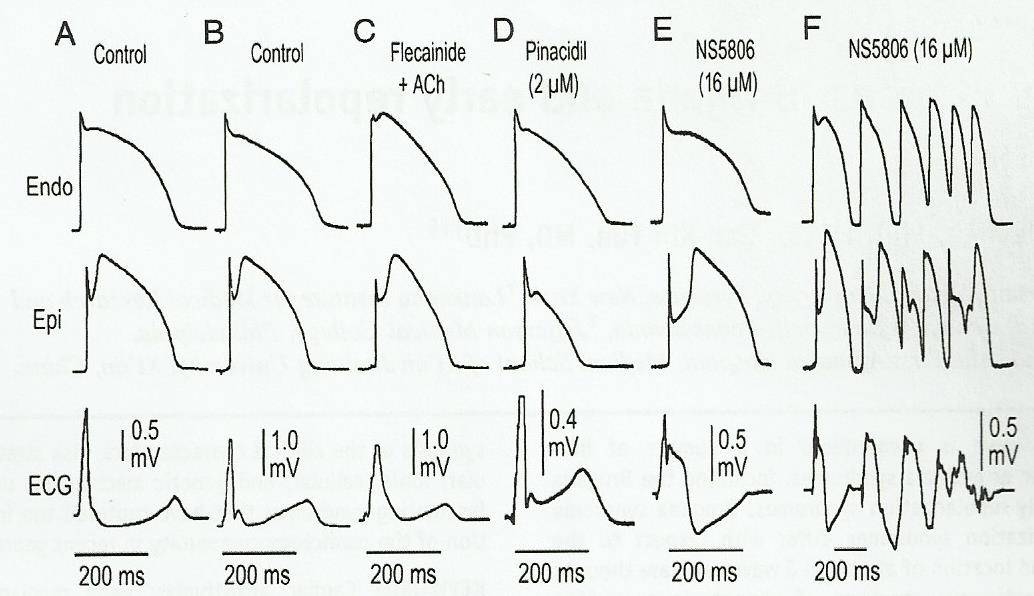
An illustration of how an ECG waveform can be generated by taking the difference between an endocardial and an epicardial potential. The tracings labelled ECG represent a transmural ECG. The transmural voltage gradients generated by the appearance of an action potential notch in the epicardium but not in the endocardium give rise to an elevated J-wave onset, JO(A), a distinct J-wave (B), slurring to the terminal part of the QRS (C), a distinct J-wave together with ST elevation (D) and a gigantic J-wave appearing as an ST segment elevation (E). ( Reproduced from Antzelevitch and Yan with permission).
Not everyone agrees with this explanation. It has been suggested that the pattern may be due to late ventricular depolarization [8,9]. There is an implication here that, in late depolarization, the QRS complex may be a little wider as would have been the case in “normal” depolarization but since QRS duration varies so much from individual to individual, it is essentially impossible to determine whether a QRS complex might be widened due to late depolarisation.
Spodick had regarded the term early repolarization as a misnomer [10]. In fact, he referred to early and late depolarisation in the same ECG by regarding a notch or slur in some leads as “early repolarisation” and ST elevation in other leads of the same ECG as “delayed depolarisation”. He regarded both features as due to the same process. He suggested that “differential repolarisation between parts of the left or both ventricles might be an explanation”. Surawicz and the author also pointed out that the term “early repolarisation” could be confusing [11].
The Confusing Years
Notwithstanding any of the above Introduction, the finding of a link between the ECG pattern termed early repolarisation and idiopathic ventricular fibrillation caused considerable excitement in the cardiological community, as might be expected. Many other researchers began to review data to see if the link could be confirmed. However, a close inspection of some of the papers that were published revealed, at least to this author, that there was a wide variation in the definition of the term “early repolarization”. This was very clearly confirmed in a review in 2013 by Maury and Rollin [12] which showed that just a few years after the publication of the 2008 paper causing all the interest [1], there were 22 studies, with 21 published between 2008 and 2013, on the prevalence of early repolarization which showed a prevalence which varied between 0.9% and 31%. Clearly, there was a considerable difference of opinion in what different authors regarded as early repolarization!
Haissaguerre Definition
The definition of ER in the paper by Haissaguerre et al [1] was “an elevation of the QRS-ST junction (J point) in at least 2 leads (within the same territory, e.g. inferior or lateral leads). The amplitude of the J point elevation had to be at least 0.1mV above the baseline level, either as QRS slurring (a smooth transition from the QRS segment to the ST segment) or notching (a positive J deflection inscribed on the S wave)”. This is a rather strange definition as the S wave by definition lies below the baseline and the earlier papers [4,6] had referred to a notch on the downslope of the R wave. The amplitude and slope of the ST segment was not part of the Haissaguerre definition. In 2009, Tikkanen et al [13] followed this definition and linked the ER pattern in the inferior leads with an increased probability of death due to cardiac causes in a 30±11 year follow up of ECGs recorded on paper around 1966-1972 in 10,864 middle aged individuals. In a subsequent paper, the same team introduced the concept of ST slope having prognostic significance in the presence of early repolarization [14].
Close inspection of the 2011 paper by Tikkanen et al [14] revealed (in their Figure 2) that the amplitude of the J point was actually measured with respect to a point “at the time point of QRS offset drawn from another lead”. This approach simply had to be different from the definition of Haissaguerre et al [1] and unique in many ways.
It is worth noting at this stage many cardiologists reported early repolarization on an ECG particularly if there was ST elevation in V4-V6 in what otherwise was a normal ECG (Figure 3). This type of definition can be seen in the textbook of Chung (1986) [15]. The definition of Haissaguerre et al [1] which did not involve ST elevation led others such as Perez et al to express concern at the potential for the Haissaguerre definition to cause over reporting of early repolarisation with the potential for large numbers of healthy individuals to be reviewed clinically with possible liability issues [16]. They wished the definition to remain similar to that of Kambara et al [6] where ST elevation was involved.
Figure 3
An ECG meeting the criteria of early repolarisation used by many cardiologists, namely marked ST elevation in V4-V6 in an otherwise normal ECG. This was the definition of Chung [15] and others.
Others such as Rosso et al regarded “J waves” or “J-point elevation” as “hump-like” deflections “immediately after a positive QRS complex” as being consistent with early repolarization [17]. In order to allow for J-point elevation inside the QRS complex, they allowed for slurring at the terminal part of the QRS complex. J point amplitude was measured from “the baseline”.
All of this confusing situation led the author to consider what was really meant by J point. Figure 4 shows, in highly schematic form, a notch at the end of a QRS complex where it could be argued that amplitudes at A, B and C could all be regarded as the J point. It was established by the author that different groups used A or B or C, i.e. all three points were regarded as the “J point” by one or more groups. Of course, it almost goes without saying that for most of the 20th Century, the J point had been regarded as the end of the QRS complex and to a significant extent still is, but if a notch is to represent early repolarization, does that mean that ventricular depolarization has completely finished in all parts of the myocardium and hence, a notch somehow or other represents the onset of repolarisation? If so, should the “J point” be the beginning of the notch at A or the peak of the notch at B? This author would regard C as the end of the QRS complex! There is good reason for choosing C if Figure 5 is considered in detail. There it can be seen that the choice of B in some leads could result in a QRS duration of approximately 50ms which is non-physiological in an adult.
Figure 4
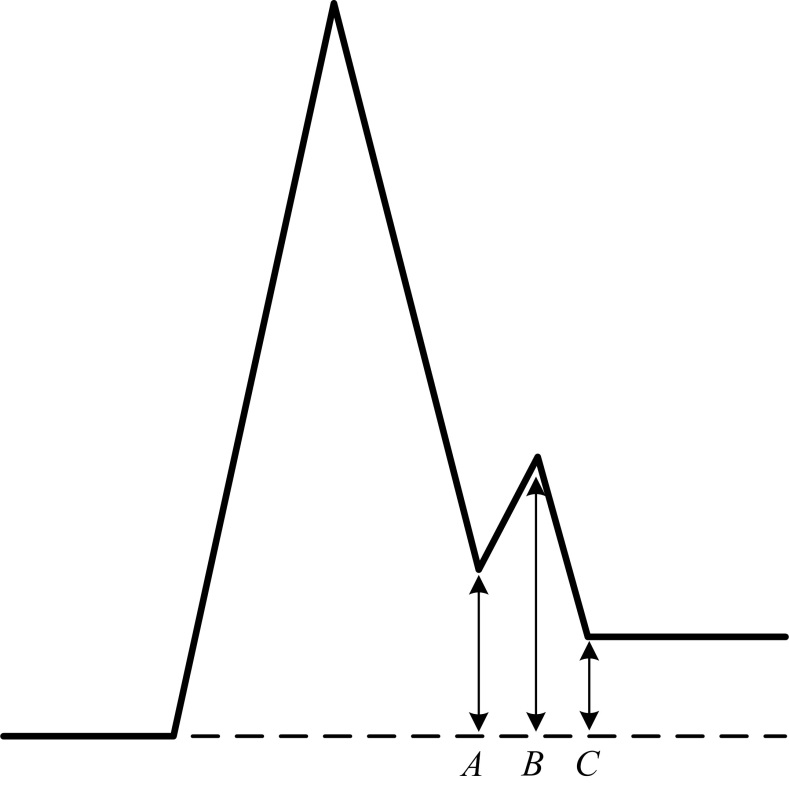
A schematic illustration of an end QRS notch with 3 points at the beginning peak and end of the notch, labelled as A, B and C respectively.
Figure 5
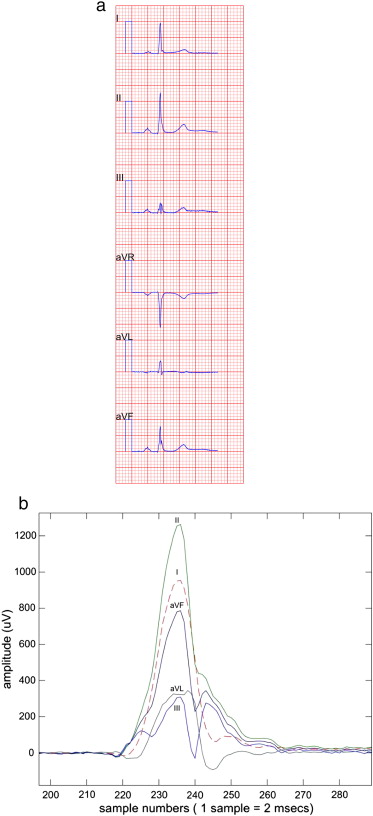
An illustration of the limb leads of an ECG, exluding aVR and an expanded digitised plot of the same leads, which show that the peak of the notch in several leads occurs approximately 50ms after QRS onset, suggesting that this could not be the end of ventricular depolarization and hence the end of the QRS complex.
Could there be a consensus?
All of this confusion led the author to consider holding a one day workshop on early repolarization on the occasion of the 40th International Congress on Electrocardiology which was held in Glasgow in August 2013. All of the principal players in this area of early repolarization were invited to the workshop and it was pleasing to note that there was representation from every group with significant publications in the area, with the exception of one as the Principal Investigator was unable to travel a long distance by air. A special collection of papers on the topic of J waves and early repolarisation was published in the September/October 2013 issue of the Journal of Electrocardiology [18] to accompany the symposium at which preprints were available.
Perhaps the most interesting point to arise from the discussion was the variation among those present as to which of A, B, C in Figure 4 should be the J point. There was support for each from different attendees. At that meeting, this author tried very hard (!) to avoid all reference to “J point” by describing the notch or slur as an end QRS notch or an end QRS slur.
It was clear that on the basis of the one day symposium, that even with a lengthy discussion, an agreement could not be reached on terminology etc. After the symposium, there followed many months of an exchange of views on the topic. Agreement was finally reached and a consensus paper on the early repolarisation pattern was published [19]. This paper aimed to produce a set of measurements that should be made by researchers working on the ER pattern so that data from different centres could be compared in future studies. For example, the onset, peak and termination of an end QRS notch were simply labelled Jo, Jp and Jt respectively (see Figure 6). The paper did not set out to define “the J point”.
Figure 6

The new definitions of the onset peak and termination of an end QRS notch and slur, labelled as Jo, Jp and Jt respectively. The onset of the notch is labelled as Jp.
( Reproduced from JACC 2015; 66: 470-7, with permission)
In the case of a slur, it was agreed that there would be only 2 points of measurement, namely the onset of the slur, which was taken to be Jp, i.e. the peak amplitude of the slur and the end of the slur, Jt.
Some additional duration measurements were added, namely D1, D2 as shown in Figure 6. These were provided in case researchers in the future wish to comment on the width of a notch or slur.
Definition of the early repolarisation pattern
The new labelling allowed the early repolarisation pattern to have the following definition.
- There is an end QRS notch or slur on the downslope of a prominent R wave. If there is a notch, it should lie entirely above the baseline. The onset of a slur must also be above the baseline.
- Jp is ≥ 0.1mV in two or more contiguous leads of the 12 lead ECG, excluding V1 to V3.
- QRS duration is < 120ms.
It should be noted that all of these measurements are referred to QRS onset which is regarded as the zero reference level. The definition allows future research to be based on all three measurements, Jo, Jp and Jt so that it is perfectly clear in any publication what the authors are using for their measurements in relation to end QRS notching and slurring. The definition is therefore independent of whether one cardiologist thinks that Jo is the end of the QRS and another thinks Jt is the end of the QRS complex. This is a very significant advantage of the new definition. Of course, the measurements can be used by researchers even if they disagree with the definition of early repolarisation quoted here. For example, if the wish to report on the significance of ST elevation in the presence of a notch or a slur, they can quote their measurements of Jt.
Figure 7 shows an ECG that meets the new, but not the “classic” definition of early repolarisation. There is end QRS notching but not any ST elevation while the QRS duration < 120ms.
Figure 7
An ECG which meets the new definition of early repolarisation with end QRS notching, Jp≥ 0.1mV and a QRSd < 120ms in V5, V6. Note that Jt < 0.1mV which is not part of the definition but which indicates that there is no ST elevation in these leads.
Given that Tikkanen and colleagues [13] as well as Rosso et al [20] had worked on the question of ST slope, the consensus group felt it was sensible to follow the definitions which had been used by Tikkanen et al. The group agreed the following.
- ST segment slope should be measured from Jt.
- The ST segment slope should be regarded as horizontal or downward sloping if the amplitude of the ST segment 100ms after Jt (interval M – Figure 8) is ≤ the amplitude at Jt. The ST segment should be regarded as upward sloping if the amplitude of the ST segment 100ms after Jt (interval M – Figure 8) > amplitude at Jt.
- If the researcher has not used Jt when measuring slope, any report must clearly state whether 100ms intervals such as K, L and M have been used (Figure 8).
Figure 8
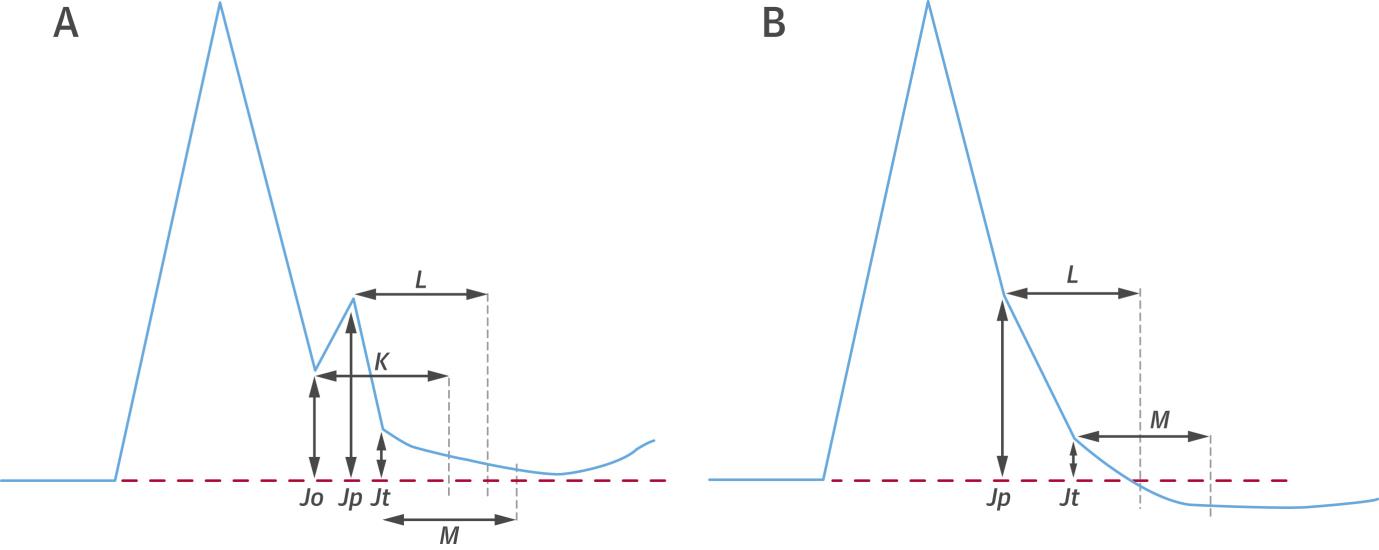
The horizontal lines, K, L, M represent 100ms intervals. It is suggested that ST slope can be measured from the beginning to the end of these intervals.
( Reproduced from JACC 2015; 66: 470-7, with permission)
Discussion
The most important point to be made at this stage is that the consensus paper sets out, clearly, measurements which require to be made when researching early repolarization as the term is currently applied. A consensus definition [19] is provided but it could well be in future that this is altered and in that case, it is hoped that the measures outlined in the consensus paper can be used, perhaps with different thresholds. As readers will be aware, it is very common in electrocardiography to use a threshold such as 0.1mV because it represents the amplitude of one small square on ECG paper. If the precision of automated ECG measurement is to be utilised, then other thresholds such as 0.125mV might be more valuable, but this is pure speculation.
The second point which can be made is that an ECG showing only relatively widespread ST elevation or even ST elevation in the lateral leads, V4-V6, particularly in an apparently healthy younger person, should no longer be reported as early repolarization. It could, for example, be regarded as non specific ST elevation, in keeping with early thoughts on the normal variant of the RS-T segment.
Thirdly, the consensus paper did not attempt to review the extensive literature on the use of wedge preparations of canine myocardium for studying repolarization. There are many excellent reviews on this topic [7]. Nor did the consensus set out in any great detail the clinical aspects of early repolarization. It did attempt to avoid creating “heart disease of electrocardiographic origin” [21] by indicating that in the absence of any symptoms such as syncope, or a strong family history of juvenile sudden cardiac death, then a pattern of end QRS notching and slurring should not be regarded as abnormal in an otherwise healthy individual. Essentially that allays the concerns of Perez et al [18].
Publications on the early repolarisation pattern continue to appear but there has been little time to acknowledge the new definition. One article in press from the Haissaguerre group [22] refers to the value of the T/R ratio in separating benign from malignant early repolarisation but those who incline to supporting the classical definition of ER [6] could say that a low T/R ratio, now regarded as a marker of malignant ER, is not consistent with what was known as early repolarisation in any event where a tall T wave was one of the criteria! In short, some might argue that this additional criterion for malignant ER is not really ER! The new school of thought does not include ST elevation in the definition of ER, a point underlined in an accompanying editorial [23] to the paper of Roten et al [22]. Strangely, this editorial [23] does not reference the new definition of ER even although two of the four authors were also authors of the consensus paper!
While new criteria take time to be assessed with respect to prognosis, established data bases can be helpful in reviewing different criteria. Another recent paper from Froelicher’s group [24] found that J waves and QRS slurs in the inferior and/or lateral leads did not provide increased risk for cardiovascular death in a 10 year follow up of 20,661 predominantly male patients.
In summary, the topic of early repolarisation pattern is still controversial and it is hoped that further studies can be facilitated by the use of the measures outlined in the consensus paper [19] irrespective of terminology regarding J waves¡
REFERENCES
- Haissaguerre M, Derval N, Sacher F, et al. Sudden Cardiac Arrest associated with Early Repolarization. N Eng J Med 2008;358:2016-23.
- Myers GB, Klein HA, Stofer BE, Hiratzka T. Normal variations in multiple precordial
leads. Am Heart J 1947; 34(6): 785-808.
- Goldman MJ. RS-T segment elevation in mid and left precordial leads as a normal
variant. Am Heart J 1953; 46(6): 817-820.
- Wasserburger RH, Alt WJ. The normal RS-T segment elevation variant. Am J Cardiol 1961; 8: 184-192.
- Grant RP, Estes HE Jr, Doyle JT. Spatial vector electrocardiography: the clinical characteristics of S-T and T vectors. Circulation 1951; 3: 182-197.
- Kambara H, Phillips J. Long-term evaluation of Early Repolarization Syndrome (normal variant RST-T Segment Elevation). Am J Cardiol 1978;38:157-181.
- Antzelevitch C, Yan GX. J-wave syndromes: Brugada and early repolarization syndromes. Heart Rhythm 2015;12:1852-66.
- Wellens H. Early repolarization revisited. N Engl J Med 2008; 358: 2063-5.
- Hoogendijk M, Potse M, Coronel R. Critical appraisal of the mechanism underlying J waves. J Electrocardiol 2013; 46: 390-4.
- Spodick D. Early repolarization: an underinvestigated misnomer. Clin Cardiol 1997; 20: 913-4.
- Surawicz B, Macfarlane PW. Inappropriate and confusing electrocardiographic terms: J wave syndromes and early repolarization. J Am Coll Cardiol 2011;7:1584-6.
- Maury P, Rollin A. Prevalence of early repolarization/J wave patterns in the normal population. J Electrocardiol 2013; 46: 411-416.
- Tikkanen JT, Anttonen O, Junttila MJ, et al. Long-term outcome associated with Early Repolarization and Electrocardiography. New Eng J Med 2009; 361: 2529-37.
- Tikkanen JT, Junttila MJ, Anttonen O, et al. Early Repolarization. Electrocardiographic Phenotypes associated with favourable long-term outcome. Circulation 2011; 123: 2666-2673.
- Chung EK. Electrocardiography: Practical Applications with Vectorial Principles. Second Edition, 1980; Harper & Row Publishers, Hagerstown, Maryland.
- Perez MV, Friday K, Froelicher V. Semantic Confusion: The case of early repolarization and the J point. Am J Med 2012; 125: 843-4.
- Rosso R., Kogan E, Belhassen B, et al. J-Point elevation in survivors of Primary Ventricular Fibrillation and matched control subjects. J Am Coll Cardiol 2008; 52: 1231-38.
- Froelicher V, Wagner G. Symposium on the J wave patterns and a J wave syndrome. J Electrocardiol 2013; 46: 381-2.
- Macfarlane PW, Antzelevitch C, Hassaguerre M, Huikuri HV, Potse M, Rosso R, Sacher F, Tikkanen JT, Wellens H. The Early Repolarization pattern: a Consensus Paper. JACC 2015; 66(4): 470-477.
- Rosso R, Glikson E, Belhassen B, Katz A, Halkin A, Steinvil A, Viskin S. Distinguishing “benign” from “malignant early repolarization”: The value of the ST-segment morphology. Heart Rhythm 2012; 9(2): 225-229.
- Marriott H. Practical Electrocardiography, 6th Edition. Williams and Wilkins, Baltimore. p266. 1977.
- Roten L, Derval N, Maury P, Mahida S, Pascale P, Leenhardt A, et al. Benign vs malignant inferolateral early repolarization: Focus on the T wave. Heart Rhythm 2015; (in press).
- Viskin S, Havakuk O, Antzelevitch C, Rosso R. Malignant Early Repolarization: It’s the T-Wave Stupid … Heart Rhythm 2015; (in press).
- Pargaonkar VS, Perez MV, Jindal A, Mathur MB, Myers J, Froelicher VF. Long-Term Prognosis of Early Repolarization with J-Wave and QRS Slur Patterns on the Resting Electrocardiogram. A Cohort Study. Annals of Internal Med 2015; 163(10): 747-758.


































4 Comments
José Luis Palma
febrero 8, 2016, 11:35 amCon la electrocardiografía de alta resolución, las muescas terminales del QRS en su unión con el ST-T se asocian en un tercio de los casos a post-potenciales tardíos oscilantes causados por una dispersión terminal del frente de onda de despolarización ventricular. En pacientes con miocardiopatía dilatada severa, sea o no de origen isquémico, es relativamente frecuente observar estos post-potenciales tardíos. Si esta anomalía induce o no mayor prevalencia de muerte súbita por arritmias ventriculares letales está aun por determinar. En cualquiera de los casos la discusión que genera la mal llamada "repolarización precoz" es muy atractiva e intrigante.
REPLYUnai Sebastien Martinez@José Luis Palma
abril 28, 2022, 11:39 amI am Unai Martinez. Thanks to DR WATER for his good work. Finally a cure for diabetes exists. It’s not a pharmaceutical drug, but a very safe all natural herbal product that restores your body’s own ability to naturally control it’s own blood glucose levels back to normal. I have been battling with diabetes type 2 for 12 years now, before a friend lead me to DR WATER. He said that he could cure just about any disease, but I never believed. I just decided to give it a try. I contact him that night luckily for me, he was online. He said yes he could heal me, but yet again I didn’t believe, I even thought it was a scam. But I went on to give it a try. He ask some question about my health and I provided him with all he needed. And a few days later, I received a call from UPS to come collect some herbal products from DR WATER. I can’t believe that after using those herbal products, I was healed and I can not stop telling people about this experience. When I went to the hospital for check up, my doctor was
REPLYsurprised and he even ask for DR WATER’s email DRWATERHIVCURECENTRE@GMAIL.COM, which i gave to him and have given alot of people. This indeed is a genuine solution to Diabetes that I am sharing here, not those very costly medical
treatment or a life-long use of diabetic supplements. If you need this herbal product, contact him now. He can still help you on other diseases like:
1, hepatitis
2, HIV
3, Herpes or any skin disease
4, asthma
5,HPV genital warts
6,Cancer
7,Ulcer
8, Chlamydia
9, shingles
10, Sclerosis
11, Arthritis
12, Fibroid, infertility, ovarians cysts, frequent miscarriages, premature ejaculation.
You can also contact him on his
whatsapp +2349050205019.
Carlos Ceballos@Unai Sebastien Martinez
abril 28, 2022, 11:40 amHappiness is all i see now, I never thought that I will see this day when i will be healed and free from this virus. My name is Ceballos, my email is carlosceballos1cb@gmail.com. I am in Santiago, Chile. I have been suffering from serious oubreakes of herpes for the past 3 years now; I had spent a lot of money going from one places to another in search of a good cure. From hospitals to hospitals, from gynacologist to another. Constant checks up have been my hobby not until this faithful day, I was searching through the internet, I saw a testimonies on how people were cured of herpes with herbal remedies. I specicifically saw the name Dr.water as the healer who that was helping to heal people with this medicine. Quickly, I copied his email which is drwaterhivcurecentre@gmail.com. Just to give him a trial. I spoke to him, he asked me for some information, which I gave him. He told me that he is going to provide the herbal medicine to me, which he did and instructed me on how to use it. I used it and indeed my outbreaks were gone. But to be full convinced that i have been healed, he asked me to go for medical checkup after some days of using the herbal product. I went for the check up and confirmed that i was free from the deadly disease. Yes i was indeed healed from herpes. To show my gratitude, he only asked me to post the testimony to tell the whole world, which i am happily doing now. please brothers and sisters, he is great, I owe him in return. And i will beg that you patronize him. if you are having a similar problem just Contact him on whatsapp; +2349050205019 or write him with the email above.
REPLYDiallo Antoine@Carlos Ceballos
abril 28, 2022, 11:42 amWhat else can I say about him, today am equally very grateful to Dr.Water as I am finally cured of HIV disease that have been eating me up for over a year and 6 months. After searching for different means to get my self cure but nothing seems to work out, behold today i can boldly stand and testify to the world at large that with the help of herbal medicine, I have found myself back to my feet and healthy again in just after few weeks after i got in contact with a great herbalist, through help on a blog which talk about HIV cure. Few weeks ago, i saw an of a lady eplainning how she was cured through the herbal medicine too which was sent to her by Dr.Water. So i decided to give this great man a try by contacting him via his email and mobile number, i explained to him what my problems his and he promised that me all would be fine and well by the time he his done with is own work. I just had to believe in him, which i did ,low and behold, today i am very happy as it was just all like a magic that is why i have come here to testify to the world at large and also to share my experience because I know there are many people out there who are also in searching for a cure to one disease or the other. You can as well get in contact with DR.WATER now for herbal medicine help through his WhatsApp +2349050205019 as i fully believe he is able and capable to cure HIV/AIDS and can also cure all of these diseases: HEPATITIS B, HPV WARTS, CANCER, hERPES SIMPLEX VIRUS, ALS, DIABETES TYPE1&2, INFERTILITY IN BOTH MALE AND FEMALE
REPLY